What are pituitary tumours?
Pituitary tumours are abnormal growths in the pituitary gland. These tumours are almost always benign (not cancerous), but can affect hormonal balance and can disrupt the normal functioning of the pituitary gland.
The two types of pituitary tumours are: secretory (makes hormones) and non-secretory (don’t make hormones). Depending on which hormone the tumour produces, a variety of imbalances can occur. If non-secretory tumours become large (1cm or larger), they can press against the pituitary gland or the brain and cause problems with normal pituitary function.
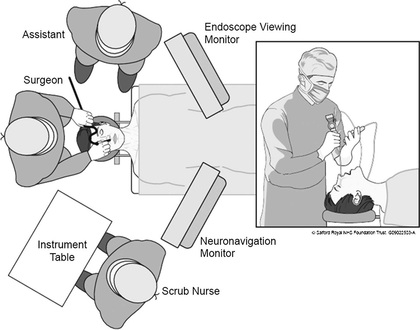
Your doctor has recommended surgery as the best treatment to remove your tumour. The pituitary gland is often best reached through one of the nostrils. This is called transsphenoidal surgery, which means “through the sphenoid sinus”.
The surgeon removes a small piece of bone to reach the pituitary gland and the tumour. The tumour is often removed using an endoscope (fine telescope). The surgery is often performed by a neurosurgeon and an otolaryngology (“ENT”) surgeon.
The goal of surgery is to relieve symptoms, confirm a diagnosis (through a pathology report), and to bring hormone levels back to normal.
Sometimes patients may develop ADH deficiency called diabetes insipidus due to damage to the pituitary after surgery. Antidiuretic hormone helps regulate water balance in the body by controlling the amount of water the kidneys reabsorb. If there is too little ADH or the kidneys do not respond to ADH, then too much water is lost through the kidneys, the urine produced is more dilute than normal, and the blood becomes more concentrated. This can cause excessive thirst, frequent urination, dehydration, and high blood sodium (hypernatremia). If there is too much ADH, then water is retained, blood volume increases, and the person may experience nausea, headaches, disorientation, lethargy, and hyponatremia. Frequently this disorder is corrected with temporary use of medication (desmopressin) during the post-operative period. In some cases, the damage can take longer to correct and you may need to continue medication for a longer period of time after surgery.
Call your doctor if you have:
1. Persistent fresh bleeding from the nose (more than a little blood stain)
2. Change in your vision (loss or double vision)
3. Neck pain, increased temperature, or sensitivity to light
4. Worsening headache or odour from the nasal cavities
5. Constant, unquenchable thirst
6. Frequent urination that is pale coloured
7. Light-headed, dizzy, or fainting
Go to the nearest Emergency Department immediately if:
1. Persistent dripping of clear, watery solution from nose
2. Drowsiness, difficult to awaken
3. Confusion, restless, nausea, and vomiting
Follow-up
You will need to see your endocrinologist within 4-6 weeks after surgery. Until this time continue any prescribed medications. Blood work will be done 1 week prior to this appointment.
You will also have an MRI, visual field testing, blood work, and a clinic visit with your neurosurgeon and endocrinologist within 3 months.
An eye doctor (ophthalmologist) will follow you after surgery.
Pituitary tumours are abnormal growths in the pituitary gland. These tumours are almost always benign (not cancerous), but can affect hormonal balance and can disrupt the normal functioning of the pituitary gland.
The two types of pituitary tumours are: secretory (makes hormones) and non-secretory (don’t make hormones). Depending on which hormone the tumour produces, a variety of imbalances can occur. If non-secretory tumours become large (1cm or larger), they can press against the pituitary gland or the brain and cause problems with normal pituitary function.
Your doctor has recommended surgery as the best treatment to remove your tumour. The pituitary gland is often best reached through one of the nostrils. This is called transsphenoidal surgery, which means “through the sphenoid sinus”.
The surgeon removes a small piece of bone to reach the pituitary gland and the tumour. The tumour is often removed using an endoscope (fine telescope). The surgery is often performed by a neurosurgeon and an otolaryngology (“ENT”) surgeon.
The goal of surgery is to relieve symptoms, confirm a diagnosis (through a pathology report), and to bring hormone levels back to normal.
Sometimes patients may develop ADH deficiency called diabetes insipidus due to damage to the pituitary after surgery. Antidiuretic hormone helps regulate water balance in the body by controlling the amount of water the kidneys reabsorb. If there is too little ADH or the kidneys do not respond to ADH, then too much water is lost through the kidneys, the urine produced is more dilute than normal, and the blood becomes more concentrated. This can cause excessive thirst, frequent urination, dehydration, and high blood sodium (hypernatremia). If there is too much ADH, then water is retained, blood volume increases, and the person may experience nausea, headaches, disorientation, lethargy, and hyponatremia. Frequently this disorder is corrected with temporary use of medication (desmopressin) during the post-operative period. In some cases, the damage can take longer to correct and you may need to continue medication for a longer period of time after surgery.
Call your doctor if you have:
1. Persistent fresh bleeding from the nose (more than a little blood stain)
2. Change in your vision (loss or double vision)
3. Neck pain, increased temperature, or sensitivity to light
4. Worsening headache or odour from the nasal cavities
5. Constant, unquenchable thirst
6. Frequent urination that is pale coloured
7. Light-headed, dizzy, or fainting
Go to the nearest Emergency Department immediately if:
1. Persistent dripping of clear, watery solution from nose
2. Drowsiness, difficult to awaken
3. Confusion, restless, nausea, and vomiting
Follow-up
You will need to see your endocrinologist within 4-6 weeks after surgery. Until this time continue any prescribed medications. Blood work will be done 1 week prior to this appointment.
You will also have an MRI, visual field testing, blood work, and a clinic visit with your neurosurgeon and endocrinologist within 3 months.
An eye doctor (ophthalmologist) will follow you after surgery.
